 New standard management options for rosacea have been published in the Journal of the American Academy of Dermatology.1 Developed by a consensus committee and review panel of 27 rosacea experts worldwide, the updated guidelines are intended to provide a comprehensive summary of treatment options for the respective signs and symptoms, also known as phenotypes, identified in the recently updated standard classification of rosacea, allowing physicians to tailor therapy for each individual case to achieve optimal patient outcomes.2
New standard management options for rosacea have been published in the Journal of the American Academy of Dermatology.1 Developed by a consensus committee and review panel of 27 rosacea experts worldwide, the updated guidelines are intended to provide a comprehensive summary of treatment options for the respective signs and symptoms, also known as phenotypes, identified in the recently updated standard classification of rosacea, allowing physicians to tailor therapy for each individual case to achieve optimal patient outcomes.2
“The growing scientific understanding of rosacea has established a consistent disease process that underlies the various potential clinical manifestations of the disorder, designated in the new standard classification system as phenotypes,” said Dr. Diane Thiboutot, professor of dermatology at the Pennsylvania State University. “At the same time, important advances in medical therapy have been developed for specific manifestations of the disorder, making multiple options available so that clear or near clear skin may be possible for increasing numbers of patients.”
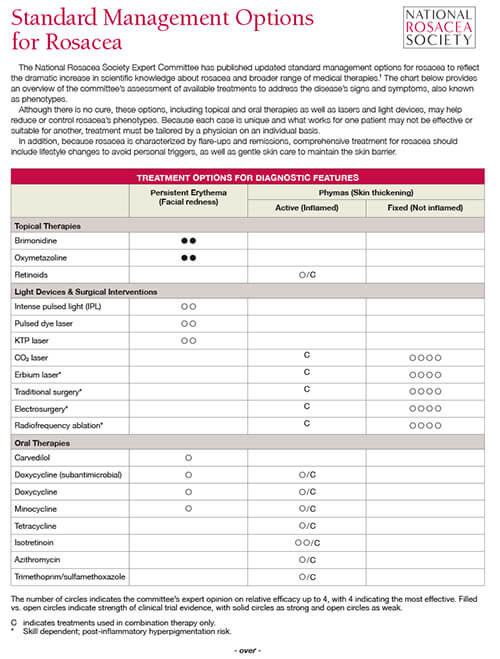
Dr. Thiboutot noted that the standard management options, listed in tables by phenotype, also include expert evaluations of effectiveness and quality of evidence to serve as a guide for providing targeted treatment and care on an individual basis. The National Rosacea Society has produced a free PDF for patients that provides an overview of the committee’s assessment of available treatments to address the disease’s signs and symptoms. Download it here.
Although the features of rosacea may appear at different times and in different combinations, research has found that all appear to be manifestations of the same underlying inflammatory continuum. Therefore, different therapies may be acting on different aspects of that continuum. Recent studies point to multiple pathogenic pathways, including defects in the innate and adaptive immune systems, mast cells and related biochemical mechanisms, and the neurovascular system. Learn more about the potential causes of rosacea.
According to the updated classification system, the presence of one of two phenotypes – persistent facial erythema or, less commonly, phymatous changes where the facial skin thickens – is considered diagnostic of rosacea. Additional major cutaneous signs, which often appear with the diagnostic features, include papules and pustules, flushing, telangiectasia and certain ocular manifestations. The presence of two or more major phenotypes independent of the diagnostic features is also considered diagnostic of rosacea. Secondary phenotypes, which must appear with one or more diagnostic or major phenotypes, include burning or stinging, swelling and dry appearance.
Signs suggestive of ocular rosacea include telangiectases on the eyelid margin and bloodshot eyes, as well as inflammation and growth of fibrous tissue on the eye. Burning, stinging, light sensitivity and the sensation of a foreign object may also occur, as well as conjunctivitis, inflammation of glands at the rim of the eyelids (blepharitis) and crusty accumulations at the base of the eyelashes.
“Although the original standard classification of rosacea designated the most common presentations as subtypes, because rosacea now appears to develop from a consistent inflammatory continuum, it seems appropriate to focus on the individual features that may result from this disease process,” Dr. Thiboutot said. “By taking into consideration the full range of potential phenotypes that may occur, the assessment of severity and the selection of treatment may be precisely tailored for each individual patient.”
While there is no cure for rosacea, the standard management options provide information on how its features can be reduced or controlled with a range of topical and oral therapies and light devices, as well as appropriate skin care and lifestyle management to avoid factors that may aggravate the condition in individual cases. Combination therapy to target the specific features is often necessary for effective treatment.
When assessing treatment, the NRS Advisory Committee noted that patients’ perception and acceptance of their facial appearance – including its impact on their emotional, social and occupational lives – may also be important in determining the level of therapy. Patient surveys have suggested that the psychosocial burden of rosacea may be substantial regardless of severity and that the goal of achieving an Investigator Global Assessment of 0 or “clear” for inflammatory papules and pustules may often be appropriate and feasible. It’s also important to remember that normalization of skin tone and color is the goal, rather than complete eradication of facial coloration, which can leave the face with a sallow appearance.
References:
1. Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol 2020;82(6):1501–1510. doi:10.1016/j.jaad.2020.01.077
2. Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol 2018 Jan;78(1):148-155. doi: 10.1016/j.jaad.2017.08.037. Epub 2017 Oct 28.